


Nhóm nghiên cứu: Majid Ahsan, Leila Babaei, Ali Gholamrezaei, and Mohammad Hassan Emami
Ngày 21/06/2011
Người phụ trách viện hàn lâm: Tony C. K. Tham
| Administration of simethicone prior to EGD reduces the amount of gastric foam and bubbles and provides better visibility for evaluating the mucosa. It also decreases the duration of endoscopy. Further trials are required to find the final effect of the drug on diagnosis of pathological lesions.1. INTRODUCTIONUpper gastrointestinal endoscopy (esophagogastroduodenoscopy or EGD) is one of the most common diagnostic and therapeutic methods of upper gastrointestinal diseases [1]. One limitation of the method is, however, the presence of air bubbles and foam in stomach and duodenum, such that it is difficult or sometimes impossible for a gastroenterologist to evaluate the mucosa using the images obtained in the presence of the bubbles. This will lead to decreased diagnostic accuracy, prolonged endoscopy time, and decreased patient’s tolerance [2]. Therefore, gastric and intestinal preparation prior to endoscopy is necessary for the removal of the bubbles.An appropriate preparation method should be able to remove the bubbles, not having side effects, be tolerable for patients, and be applicable for most patients in different conditions [3].Currently, except fasting prior to endoscopy, no standard method has been recommended for prior EGD preparation. Although some specialists routinely administer simethicone for endoscopy preparation [4].Simethicone is a detergent, which is a chemical mixture of dimethyl polysiloxane and silicagel. It is physiologically inactive and nontoxic. It can be taken orally and cannot be absorbed through gastrointestinal system [5]. By reducing the adhesion force of air bubbles, simethicone removes the bubbles. Thus, it is expected that the drug can be used for removing gastric and duodenal foams and bubbles [5]. Simethicone does not have any known drug interaction, and no significant complication has been reported for it. Therefore, the drug has been used for treatment of patients with vague abdominal complaints (because of large amount of gases), and positive effects have been observed [6].Moreover, the drug (in solution formulation) has been used in some studies for intestinal preparation prior to colonoscopy and capsule endoscopy [7]. However, thus far, no reliable report for routine use of the drug in preparation prior to EGD was available. Thus, we have evaluated the effect of simethicone on the reduction of foam and air bubbles during upper gastrointestinal endoscopy.2. METHODSThis randomized, placebo-controlled, double-blinded (patients and physician), clinical trial was carried out on patients above 18, who referred to Poursina Hakim Clinic, Isfahan (IRAN), for elective EGD. Considering the study power as to be 80% and determining the type I error as 0.05, and also setting the minimum expected difference in average of foam/air bubbles between the two groups as 0.4, according to the available data [8], and also assuming 10% for missing probability, the sample size for each group determined to be 80. The study was approved by the Ethical Committee of Isfahan University of Medical Sciences, and all patients signed an informed written consent.The sampling was carried out subsequently, and the participants were assigned to the simethicone or placebo groups randomly (according to the computer-generated table of random numbers) [9]. Fifteen to 30 minutes before EGD, in the presence of the researcher, the patients chewed a simethicone (40 mg) or placebo tablet, and then took 30 mL of water. | Việc nhai simethicone trước nội soi làm giảm lượng bọt khí và bong bóng khí trong dạ dày và cung cấp khả năng quan sát tốt hơn để đánh giá niêm mạc. Nó cũng làm giảm thời gian nội soi. Cần thử nghiệm thêm để tìm ra hiệu quả cuối cùng của thuốc trong việc chẩn đoán các tổn thương bệnh lý.1. GIỚI THIỆUNội soi đường tiêu hóa trên (esophagogastroduodenoscopy hoặc EGD) là một trong những phương pháp chẩn đoán và điều trị phổ biến nhất của các bệnh đường tiêu hóa trên [1]. Một hạn chế của phương pháp là sự hiện diện của bọt khí và bong bóng khí trong dạ dày và tá tràng đôi khi khó khăn cho một bác sĩ chuyên khoa dạ dày ruột vì không thể sử dụng các hình ảnh thu được mà có sự hiện diện của các bong bóng để đánh giá niêm mạc. Điều này sẽ dẫn đến giảm độ chính xác chẩn đoán, thời gian nội soi kéo dài, và giảm sức chịu đựng của bệnh nhân [2]. Do đó, chuẩn bị dạ dày và ruột bằng cách loại bỏ các bong bóng khí trước khi nội soi.Một phương pháp chuẩn bị thích hợp sẽ có thể loại bỏ các bong bóng, không có tác dụng phụ, thích hợp cho các bệnh nhân và được áp dụng cho hầu hết các bệnh nhân trong điều kiện khác nhau [3].Hiện nay, ngoại trừ việc nhịn ăn trước nội soi, không có phương pháp chuẩn nào được khuyến cáo cho việc chuẩn bị trước nội soi. Mặc dù một số chuyên gia thường chỉ định simethicone để chuẩn bị nội soi [4].Simethicone là một chất tẩy rửa, là một hỗn hợp hóa học của dimethyl polysiloxan và silicagel. Đó là một chất trơ về sinh lí và không độc hại. Nó có thể được uống và không thể hấp thu qua hệ tiêu hóa [5]. Bằng cách giảm lực bám dính của bọt khí, simethicone loại bỏ các bong bóng khí. Do đó, người ta cho rằng nó có thể được sử dụng để loại bỏ bọt khí và bong bóng khí trong dạ dày và tá tràng [5]. Simethicone không có bất kỳ tương tác thuốc nào, và không có báo cáo về biến chứng đáng kể nào được báo cáo. Do đó, thuốc đã được sử dụng để điều trị cho bệnh nhân đau bụng không rõ nguyên nhân (vì lượng lớn khí), và người ta đã thấy hiệu quả rõ ràng [6].Hơn nữa, thuốc (ở dạng dung dịch) đã được sử dụng trong một số nghiên cứu chuẩn bị ruột trước khi nội soi đại tràng và nội soi viên nang* [7]. Tuy nhiên, cho đến nay, không có báo cáo đáng tin cậy nào cho việc sử dụng thường xuyên thuốc để chuẩn bị trước khi nội soi là giá trị. Vì vậy, chúng tôi đã đánh giá hiệu quả của simethicone trên việc giảm bọt và bọt khí trong nội soi phần trên dạ dày ruột.2. PHƯƠNG PHÁPCác thực nghiệm ngẫu nhiên, dùng giả dược có kiểm soát, phương pháp mù đôi (bệnh nhân và bác sĩ), thử nghiệm lâm sàng được thực hiện trên bệnh nhân trên 18 tuổi, những người đã được chọn lựa bởi Poursina Hakim Clinic, Isfahan (IRAN) cho việc nội soi. Xem xét giá trị nghiên cứu là 80% và xác định lỗi loại I là 0,05, và cũng thiết lập mức độ sai biệt mong muốn tối thiểu trung bình của bọt khí/ bong bóng khí giữa hai nhóm là 0,4, theo dữ liệu có sẵn [8], và cũng giả định xác suất 10% bị thiếu, kích thước mẫu cho mỗi nhóm xác định là 80. Nghiên cứu đã được Ủy ban đạo đức của Đại học Khoa học Y khoa Isfahan phê duyệt và tất cả bệnh nhân đã ký một văn bản chấp thuận.Việc lấy mẫu đã được thực hiện sau đó, và những người tham gia được chỉ định ngẫu nhiên vào nhóm dùng simethicone hoặc dùng giả dược (theo bảng ngẫu nhiên do máy tính tạo ra) [9]. 15 đến 30 phút trước khi nội soi, với sự hiện diện của nhà nghiên cứu, bệnh nhân nhai một viên simethicone (40 mg) hoặc viên thuốc giả dược, và sau đó uống 30 mL nước. |
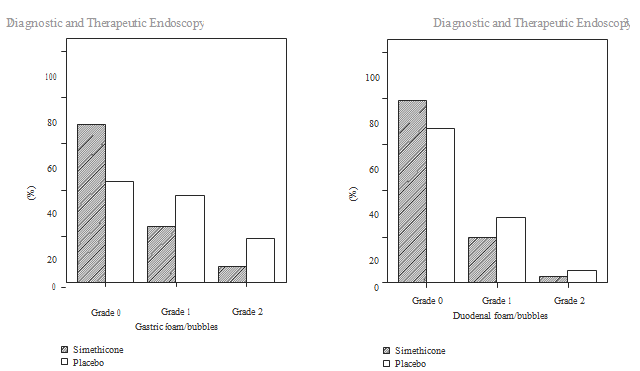
Figure 1: Comparison of the amount of gastric foam Figure 2: Comparison of the amount of duodenal foam/air bubbles between the
two groups./air bubbles between the two groups
Hình 1: So sánh tổng lượng bọt khí trong dạ dày giữa 2 nhóm Hình 2: So sánh tổng lượng bọt khí trong tá tràng giữa 2 nhóm
| Shape, box, and the route of administration of the drug were the same for the two groups. The placebo was prepared in the Pharmacy School of Isfahan University of Medical Sciences from corn starch and in the form and color of simethicone tablet.Regarding the previous studies [10, 11], we used a 4- point scale to separately measure the amount of gastric and duodenal foam/air bubbles; (0) no air bubbles, (1) there was a small amount of bubbles, without interfering in the evaluation, (2) there was a considerable amount of air bub- bles and foam, such that it was somehow difficult to evaluate, and (3) mucosal evaluation was hardly possible owing to the presence of foam and air bubbles. The amount of foam and air bubbles was recorded immediately at the end of endoscopy procedure by the gastroenterologist. The duration of the endoscopy procedure was also measured and recorded. If there was a stenosis in the upper gastrointestinal tract, such that gastric or duodenal evaluation was not possible or the stenosis led to a prolonged procedure, the patient was excluded from the study.Moreover, after carrying out the procedure, the participants’ satisfaction with the endoscopy procedure was scored on a numerical scale, in which 0 showed the least satisfaction level and 10 showed complete satisfaction. The data was analyzed by SPSS software, v. 16.0, using Chi-square test and independent sample t-test. In case of lack of normal distribution for quantitative data, we used Mann-Whitney test for comparison of the two groups. | Hình dạng viên, hộp thuốc, và cách uống thuốc là như nhau cho hai nhóm. Các giả dược đã được chuẩn bị trong trường Dược của Đại học Khoa học Y khoa Isfahan từ tinh bột ngô dựa theo hình dạng và màu sắc của viên simethicone.Theo các nghiên cứu trước đây [10, 11], chúng tôi đã sử dụng thang đo 4 điểm để đo lường riêng lượng bọt khí/ bong bóng khí trong dạ dày và tá tràng; (0): là không có bong bóng khí, (1): là có một lượng nhỏ bong bóng, mà không can thiệp vào việc đánh giá, (2): là có một lượng bọt khí và bọt đáng kể, mà khó để đánh giá, và (3): là việc đánh giá niêm mạc hầu như là không thể do sự hiện diện của bọt và bong bóng khí. Lượng bọt và bong bóng khí được ghi lại ngay lập tức bởi bác sĩ chuyên khoa tiêu hóa vào cuối thủ thuật nội soi. Thời gian của thủ tục nội soi cũng được đo và ghi lại.Nếu có một khoảng hẹp ở phần trên ống tiêu hóa, như vậy thì việc đánh giá dạ dày hoặc tá tràng là không thể hoặc khoảng hẹp dẫn đến kéo dài thực nghiệm thì các bệnh nhân đó đã được loại trừ khỏi nghiên cứu.Hơn nữa, sau khi thực hiện quy trình, sự hài lòng của người tham gia với thủ tục nội soi đã được ghi trên thang điểm số, trong đó 0 cho thấy mức độ hài lòng thấp nhất và 10 cho thấy sự hài lòng hoàn toàn. Dữ liệu được phân tích bằng phần mềm SPSS, v 16.0, sử dụng phép thử Chi-square và kiểm tra mẫu t độc lập. Trong trường hợp thiếu sự phân bố bình thường cho dữ liệu định lượng, chúng tôi đã sử dụng thử nghiệm Mann-Whitney để so sánh hai nhóm. |
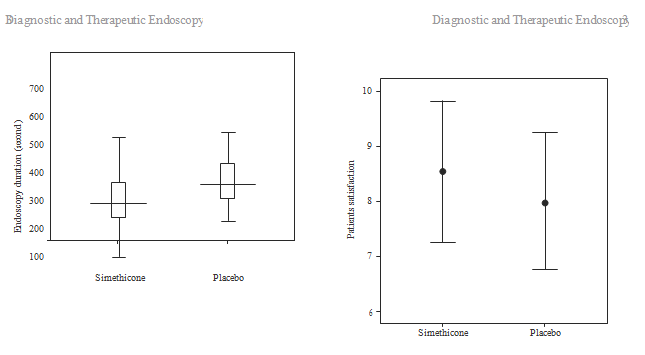
Figure 3: Comparison of the endoscopy duration Figure 4: Comparison of the patients’ satisfaction with the proce- dure between the two groups
Hình 3. So sánh về thời gian nội soi giữa 2 nhóm Hình 4. Sự hài lòng của bệnh nhân với quy trình
Sử dụng Simethicone đem lại nhiều lợi ích khi nội soi ống tiêu hóa
| 3. RESULTSWe included 90 and 83 patients in the simethicone and placebo groups, respectively. The two groups were similar in terms of age and sex. Comparison of the amount of gastric and duodenal foam/air bubbles in the two groups is demonstrated in Figures 1 and 2. In the two groups, the amount of gastric and duodenal foam/air bubbles was limited to grade 2. The amount of gastric foam/air bubbles was significantly lower in the simethicone group, compared with that of the placebo group (P = 0.002). However, the two groups were not significantly different with regard to the amount of duodenal foam/air bubbles (P = 0.422).Comparison of the two groups with respect to the duration of endoscopy procedure is demonstrated in Figure 3. The duration of endoscopy procedure was one minute shorter in the simethicone group (308.0 ± 116.2 versus 376 ± 108.1 seconds, P < 0.001).Comparison of the two groups with respect to the patients’ satisfaction with the endoscopy procedure is shown in Figure 4. The two groups were not significantly different in this regard (P = 0.646).We did not observe any severe medical complication like allergic reactions in the simethicone group.4. DISCUSSIONThe aim of the study was to determine the effectiveness of simethicone in the preparation prior to EGD. According to the results obtained, simethicone decreased the amount of gastric air bubbles and foam significantly but has no significant effect on the amount of duodenal air bubbles and foam. Another noteworthy finding was the decrease in the endoscopy procedure duration by one minute on average in the simethicone group. However, simethicone did not affect the patients’ satisfaction with the procedure. Lack of significant effect on duodenal air bubbles and foams can be due to the small amount of duodenal air bubbles during the procedure, such that only 2.4% of all patients had grade 2 of air bubbles, and, therefore, a larger sample size is required to evaluate the effect of simethicone in this respect.In addition, if we want the drug reaching duodenum, a larger amount of water is required to be taken with the drug. Moreover, in timing the drug administration, we should take into account the lagging in emptying gastric content into the duodenum.According to our literature review, there was only one report available on the effectiveness of simethicone versus placebo in preparation prior to EGD, and most studies evaluated the effectiveness of adding simethicone to the colonoscopy or capsule endoscopy preparation regimens [7]. In the study carried out by Keeratichananont et al., 121 candidates of EGD received simethicone (2 mL) or placebo solution with 60 mL of water, 15 to 30 minutes prior to EGDThey observed a decrease in the amount of esophageal, gastric, and duodenal air bubbles and foam in the simethicone group. Moreover, patients and physicians in the simethicone group were more satisfied with the procedure. However, the drug did not influence the duration of endoscopy procedure[12]. Therefore, it seems that if we want the sufficient amount of drug to reach the duodenum, a larger amount of water should be taken with the drug. According to the review and meta-analysis carried out by Wu et al. on 13 placebo- controlled studies on the effectiveness of simethicone in capsule endoscopy and colonoscopy, simethicone significantly decreases the amount of air bubbles and foams in the endoscopy field leading to an increase visibility. This provides a better chance for more accurate evaluation of the mucosa.However, the final effect of the drug on the diagnosis of pathological lesions is not investigated yet [7].In spite of being placebo-controlled, and also random- ization, and an appropriate sample size, the present study had some limitations. The amount of air bubbles and foam was evaluated by a single person (the endoscopist), on a 0–4 scale. It was better to carry out the evaluation on the basis of image processing and quantitative scales, to completely remove measurement errors and biases. Furthermore, it is not known to what extent a decrease in the amount of air bubbles and foam, and an increase in the quality of mucosal images will improve diagnosis of pathological lesions during endoscopy. Further studies are required in this respect.5. CONCLUSIONUsing simethicone prior to upper gastrointestinal endoscopy significantly reduces the amount of air bubbles and foam and increase the visibility during the procedure. This provides the possibility of more accurate evaluation of the mucosa and also decreases the endoscopy duration. We suggest comparison of effectiveness of different doses, timing of administration, and volume of simultaneous liquid, as well as the final effect of the drug on diagnosis of pathological lesions in future studies. | 3. KẾT QUẢChúng tôi đã bao gồm cả 90 và 83 bệnh nhân trong nhóm simethicone và giả dược tương ứng. Hai nhóm tương tự nhau về độ tuổi và giới tính. So sánh lượng bọt khí và bong bóng khí trong dạ dày và tá tràng ở hai nhóm được thể hiện trong hình 1 và 2. Trong hai nhóm, lượng bọt khí và bong bóng khí trong dạ dày tá tràng bị hạn chế ở mức 2. Lượng bọt khí/ bong bóng khí trong dạ dày thấp hơn đáng kể trong nhóm dùng simethicone so với nhóm giả dược (P = 0,002). Tuy nhiên, hai nhóm không có khác nhau đáng kể so với lượng bọt khí trong tá tràng (P = 0,422).So sánh hai nhóm liên quan tính đến sự kéo dài của thủ thuật nội soi được thể hiện trong hình 3. Thời gian phẫu thuật nội soi ngắn hơn một phút trong nhóm dùng simethicone (308,0 ± 116,2 so với 376 ± 108,1 giây, P <0,001).So sánh hai nhóm đối với sự hài lòng của bệnh nhân với thủ thuật nội soi được thể hiện trong Hình 4. Hai nhóm không khác nhau đáng kể về mặt này (P = 0,646).Chúng tôi đã không quan sát thấy bất kỳ biến chứng y tế nghiêm trọng nào như phản ứng dị ứng trong nhóm dùng simethicone.4. THẢO LUẬNMục đích của nghiên cứu là xác định hiệu quả của simethicone trong quá trình chuẩn bị trước khi nội soi. Theo kết quả thu được, simethicone làm giảm lượng bọt khí và bong bóng đáng kể trong dạ dày nhưng không có hiệu quả đáng kể về lượng bọt khí trong tá tràng. Một phát hiện đáng chú ý khác là giảm thời gian thủ thuật nội soi trung bình một phút trong nhóm dùng simethicone. Tuy nhiên, simethicone không ảnh hưởng đến sự hài lòng của bệnh nhân với quy trình này. Thiếu tính hiệu quả đáng kể đối với bọt khí và bong bóng khí trong tá tràng có thể là do lượng bọt khí tá tràng nhỏ trong quá trình nội soi, chỉ có 2,4% số bệnh nhân ở mức 2 về bong bóng khí, và do đó, cần có cỡ mẫu lớn hơn để đánh giá hiệu quả của simethicone ở khía cạnh này.Ngoài ra, nếu chúng ta muốn thuốc đi đến tá tràng, cần phải dùng lượng nước nhiều hơn khi uống thuốc. Hơn nữa, trong thời gian dùng thuốc, chúng ta nên tính đến thiếu việc làm rỗng phân trong dạ dày vào tá tràng.Theo đánh giá về tài liệu của chúng tôi, chỉ có một báo cáo có giá trị về tính hiệu quả của simethicone so với giả dược để chuẩn bị trước nội soi, và hầu hết các nghiên cứu được đánh giá về tính hiệu quả của việc thêm simethicone vào nội soi đại tràng hoặc phác đồ chuẩn bị nội soi viên nang [7]. Trong nghiên cứu được tiến hành bởi Keeratichananont và cộng sự, 121 người thử nội soi đã nhận được simethicone (2 mL) hoặc dung dịch giả dược với 60 ml nước, 15 đến 30 phút trước nội soi.Họ quan sát thấy sự sụt giảm lượng bọt khí thực quản, dạ dày và tá tràng trong nhóm dùng simethicone. Hơn nữa, bệnh nhân và bác sĩ trong nhóm simethicone hài lòng hơn với quy trình. Tuy nhiên, thuốc không ảnh hưởng đến thời gian của thủ thuật nội soi[12]. Do đó, có vẻ như nếu chúng ta muốn lượng thuốc đủ để tiếp cận tá tràng, nên uống thuốc với nhiều nước hơn. Theo đánh giá và phân tích tổng hợp được thực hiện bởi Wu và cộng sự, trên 13 nghiên cứu đối chứng giả dược về tính hiệu quả của simethicone trong nội soi viên nang và nội soi đại tràng, simethicone giảm đáng kể lượng bọt khí và bong bóng khí trong khi nội soi dẫn đến tăng khả năng quan sát. Điều này cung cấp một cơ hội tốt hơn để đánh giá chính xác hơn về niêm mạc.Tuy nhiên, hiệu quả cuối cùng của thuốc trong việc chẩn đoán tổn thương bệnh lý chưa được nghiên cứu [7].Mặc dù giả dược được kiểm soát cùng với lấy mẫu ngẫu nhiên, và một cỡ mẫu thích hợp, nghiên cứu này có một số hạn chế. Lượng bọt khí và bong bóng khí được đánh giá bởi một người (nhân viên nội soi), trên thang điểm 0-4. Tốt hơn là nên tiến hành đánh giá trên cơ sở xử lý hình ảnh và quy mô định lượng, để loại bỏ hoàn toàn các sai số đo lường và sai lệch. Hơn nữa, không biết đến mức độ giảm lượng bọt khí và bong bóng khí, và sự gia tăng chất lượng của hình ảnh niêm mạc sẽ cải thiện việc chẩn đoán các tổn thương bệnh lý trong suốt quá trình nội soi. Cần nghiên cứu thêm về khía cạnh này.5. KẾT LUẬNSử dụng simethicone trước khi nội soi đường tiêu hóa trên làm giảm đáng kể lượng bọt khí và bong bóng khí và tăng khả năng quan sát trong quá trình nôi soi. Điều này cung cấp khả năng đánh giá chính xác hơn về niêm mạc và cũng làm giảm thời gian nội soi. Chúng tôi đề nghị so sánh hiệu quả của các liều khác nhau, thời gian sử dụng và lượng dịch đồng thời, cũng như hiệu quả cuối cùng của thuốc khi chẩn đoán các tổn thương bệnh lý trong các nghiên cứu trong tương lai. |
70, 2008.
[3] R. Enns, “Capsule endoscopy: in search of the ideal image,”American Journal of Gastroenterology, vol. 103, no. 1, pp. 83–85, 2008.
[4] B. S. Lewis and P. Swain, “Capsule endoscopy in the evaluation of patients with suspected small intestinal bleeding: results of a pilot study,” Gastrointestinal Endoscopy, vol. 56, no. 3, pp.349–353, 2002. [5] L. Brecevic, I. Bosan-Kilibarda, and F. Strajnar, “Mechanism of antifoaming action of simethicone,” Journal of Applied Toxicology, vol. 14, no. 3, pp. 207–211, 1994. [6] G. Holtmann, J. Gschossmann, P. Mayr, and N. J. Talley, “A randomized placebo-controlled trial of simethicone and cisapride for the treatment of patients with functional dyspep- sia,” Alimentary Pharmacology and Therapeutics, vol. 16, no. 9, pp. 1641–1648, 2002. [7] L. Wu, Y. Cao, C. Liao, J. Huang, and F. Gao, “Systematic review and meta-analysis of randomized controlled trials of Simethicone for gastrointestinal endoscopic visibility,” Scandinavian Journal of Gastroenterology, vol. 46, pp. 227–235,2010. [8] R. H. Sudduth, S. DeAngelis, K. E. Sherman, and P. R. McNally, “The effectiveness of simethicone in improving visibilityduring colonoscopy when given with a sodium phosphate solution: a double-blind randomized study,” Gastrointestinal Endoscopy, vol. 42, no. 5, pp. 413–415, 1995.
[9] M. Saghaei, “Random allocation software for parallel group randomized trials,” BMC Medical Research Methodology, vol.4, article 26, 2004.
[10] B. Banerjee, J. Parker, W. Waits, and B. Davis, “Effectiveness of preprocedure simethicone drink in improving visibility duringesophagogastroduodenoscopy: a double-blind, randomized study,” Journal of Clinical Gastroenterology, vol. 15, no. 3, pp.
264–265, 1992.
[11] G. Bertoni, C. Gumina, R. Conigliaro et al., “Randomized placebo-controlled trial of oral liquid simethicone prior to upper gastrointestinal endoscopy,” Endoscopy, vol. 24, no. 4, pp. 268–270, 1992. [12] S. Keeratichananont, A. Sobhonslidsuk, T. Kitiyakara, N.Achalanan, and S. Soonthornpun, “The role of liquid sime- thicone in enhancing endoscopic visibility prior to esoph- agogastroduodenoscopy (EGD): a prospective, randomized, double-blinded, placebo-controlled trial,” Journal of the Medi- cal Association of Thailand, vol. 93, no. 8, pp. 892–897, 2010




Không có bình luận